
Rivera-Cisneros AE, Sánchez-González Jorge Manuel, Murguía-Cánovas G, Moran Moguel María Cristina, Martínez-Campos-Francisco, Martínez-Vega Karen Rubí, Lara-Mayorga Y, Vargas-Sánchez G, Noriega Muro I, Lara-Gonzalez AM, Cóccaro-Pinazo C, Ordóñez-Vázquez E, Ontiveros-Aréchiga Carrillo Oscar Adrián; Portillo Gallo Jorge H; Franco Santillán Rafael; Camacho Silvas Luis A
Introduction: Cardiometabolic risk represents a cluster of metabolic and cardiovascular abnormalities including obesity, hypertension, dyslipidemia, insulin resistance, and chronic inflammation that substantially increase the likelihood of cardiovascular disease, type 2 diabetes, and premature mortality. Evidence accumulated over the past two decades indicates that cardiometabolic risk factors frequently originate during childhood, adolescence, and early adulthood. Educational institutions represent strategic environments for preventive health interventions because they concentrate large populations and allow systematic implementation of health promotion strategies.
Objetive: The aim of this systematic review was to synthesize the scientific literature published between 2000 and 2025 addressing cardiometabolic risk within educational communities, including students, faculty members, and administrative personnel.
Material and methods: A systematic review following PRISMA 2020 guidelines was conducted. Studies were retrieved from PubMed, Scopus, Web of Science, SciELO, and Google Scholar.
Results: Eligible studies included epidemiological investigations, systematic reviews, meta-analyses, and institutional intervention studies involving educational populations. A total of 1,842 records were identified, and 96 studies met the final inclusion criteria.
Discussion: Evidence indicates increasing prevalence of cardiometabolic risk factors among adolescents and young adults, including obesity, hypertension, dyslipidemia, insulin resistance, and sedentary behavior. Institutional interventions focusing on physical activity promotion, nutrition improvement, and behavioral lifestyle interventions demonstrated reductions in cardiometabolic risk indicators ranging from 10–35%.
Conclusion: Educational institutions represent critical platforms for preventive health strategies across multiple population groups. The implementation of integrated Healthy School and Healthy University frameworks may represent effective approaches for reducing cardiometabolic risk and promoting long-term population health.
Introducción: El riesgo cardiometabólico representa un conjunto de anomalías metabólicas y cardiovasculares, incluyendo obesidad, hipertensión, dislipidemia, resistencia a la insulina e inflamación crónica, que aumentan sustancialmente la probabilidad de enfermedad cardiovascular, diabetes tipo 2 y mortalidad prematura. La evidencia acumulada durante las últimas dos décadas indica que los factores de riesgo cardiometabólico se originan frecuentemente durante la infancia, la adolescencia y la adultez temprana. Las instituciones educativas representan entornos estratégicos para las intervenciones de salud preventiva, ya que concentran grandes poblaciones y permiten la implementación sistemática de estrategias de promoción de la salud.
Objetivo: El objetivo de esta revisión sistemática fue sintetizar la literatura científica publicada entre 2000 y 2025 que aborda el riesgo cardiometabólico dentro de las comunidades educativas, incluyendo estudiantes, miembros del profesorado y personal administrativo.
Materiales y método: Se realizó una revisión sistemática siguiendo las directrices PRISMA 2020. Los estudios se recuperaron de PubMed, Scopus, Web of Science, SciELO y Google Scholar.
Resultados: Los estudios elegibles incluyeron investigaciones epidemiológicas, revisiones sistemáticas, meta-análisis y estudios de intervención institucional que involucran poblaciones educativas. Se identificaron un total de 1842 registros y 96 estudios cumplieron con los criterios de inclusión finales.
Discusión: La evidencia indica una prevalencia creciente de factores de riesgo cardiometabólico entre adolescentes y adultos jóvenes, incluyendo obesidad, hipertensión, dislipidemia, resistencia a la insulina y sedentarismo. Las intervenciones institucionales centradas en la promoción de la actividad física, la mejora de la nutrición y las intervenciones conductuales en el estilo de vida demostraron reducciones en los indicadores de riesgo cardiometabólico que oscilaron entre el 10 % y el 35 %.
Conclusión: Las instituciones educativas representan plataformas fundamentales para las estrategias de salud preventiva en diversos grupos poblacionales. La implementación de marcos integrados de Escuelas Saludables y Universidades Saludables puede representar enfoques eficaces para reducir el riesgo cardiometabólico y promover la salud poblacional a largo plazo.
Cardiovascular diseases remain the leading cause of mortality worldwide, accounting for approximately 17.9 million deaths annually, representing nearly one third of global mortality (World Health Organization, 2023)25. These diseases are strongly associated with metabolic abnormalities collectively known as cardiometabolic risk. Cardiometabolic risk encompasses several physiological disturbances including central adiposity, hypertension, dyslipidemia, insulin resistance, and impaired glucose metabolism (Grundy, 2016)13. These conditions frequently cluster together, accelerating the development of atherosclerosis and metabolic disease.
Historically, cardiometabolic diseases were considered disorders of middle and late adulthood (Carnethon, 2012; Barquera et al, 2018;)4,5. However, epidemiological evidence from longitudinal studies has demonstrated that many risk factors originate earlier in life. The Bogalusa Heart Study demonstrated that cardiovascular risk factors identified in childhood are associated with early development of atherosclerotic lesions (Berenson et al., 2015)5. Similarly, the Cardiovascular Risk in Young Finns Study showed that childhood metabolic risk factors predict adult vascular changes (Raitakari et al., 2003)26.
Adolescence and early adulthood represent critical stages in the life-course trajectory of cardiometabolic disease. Behavioral factors such as reduced physical activity, sedentary behavior, poor dietary patterns, and psychosocial stress frequently emerge during this stage (Keating et al., 2017)17.
Educational institutions therefore represent important settings for preventive health interventions (Juonala, et al, et al)16. Schools and universities provide structured environments where lifestyle interventions can be implemented systematically.
The World Health Organization introduced the concept of Health Promoting Schools, emphasizing integrated approaches that combine healthy environments, health education, community participation, and institutional policy (WHO, 2021-2023)34,35. Similarly, the concept of Health Promoting Universities extends these principles to higher education institutions (Dooris, et al., 2018; Ekelund et al, 2019)10,11.
Despite these initiatives, cardiometabolic risk continues to increase among adolescents and young adults. Moreover, limited research has examined cardiometabolic health among faculty members and administrative staff, who may experience increased risk due to sedentary occupational environments (Ford et al, 2002; Hu, 2011; Hallal et al, 2012)12,14,15.
Therefore, a systematic review of available evidence is necessary to better understand cardiometabolic risk patterns within educational communities.
Study Design
This study followed PRISMA 2020 guidelines for systematic reviews (Page et al., 2021)24.
Databases Searched
PubMed / MEDLINE; Scopus; Web of Science; SciELO; Google Scholar.
Search period
January 2000 – December 2025.
Keywords included
Cardiometabolic risk; metabolic syndrome; cardiovascular risk factors; health promoting schools; health promoting universities; university student; physical activity intervention. Spanish equivalents were also used.
Inclusion Criteria
Studies were included if they: Were published between 2000–2025; included educational populations; evaluated cardiometabolic indicators; examined health promotion interventions.
Exclusion Criteria
Studies were excluded if they: Did not involve educational populations; did not measure cardiometabolic variable; were editorials or commentaries.
Study Characteristics
The Figure 1 shows the data the systematic search identified 1,842 records, of which 96 studies met the inclusion criteria after screening and eligibility assessment according to PRISMA guidelines (Page et al., 2021)24.
The included studies were conducted across multiple geographic regions, including North America, Europe, Latin America, and Asia. The majority of studies were observational cross-sectional investigations evaluating cardiometabolic risk factors in educational populations. Several studies also evaluated intervention programs designed to improve physical activity levels, dietary behaviors, or overall lifestyle patterns within educational institutions.
The populations analyzed in the included studies encompassed three main groups within educational communities: Students (secondary and university level); faculty members; administrative personnel. Most studies focused primarily on students, representing approximately 65% of included investigations, while fewer studies assessed cardiometabolic health among faculty members or administrative staff.
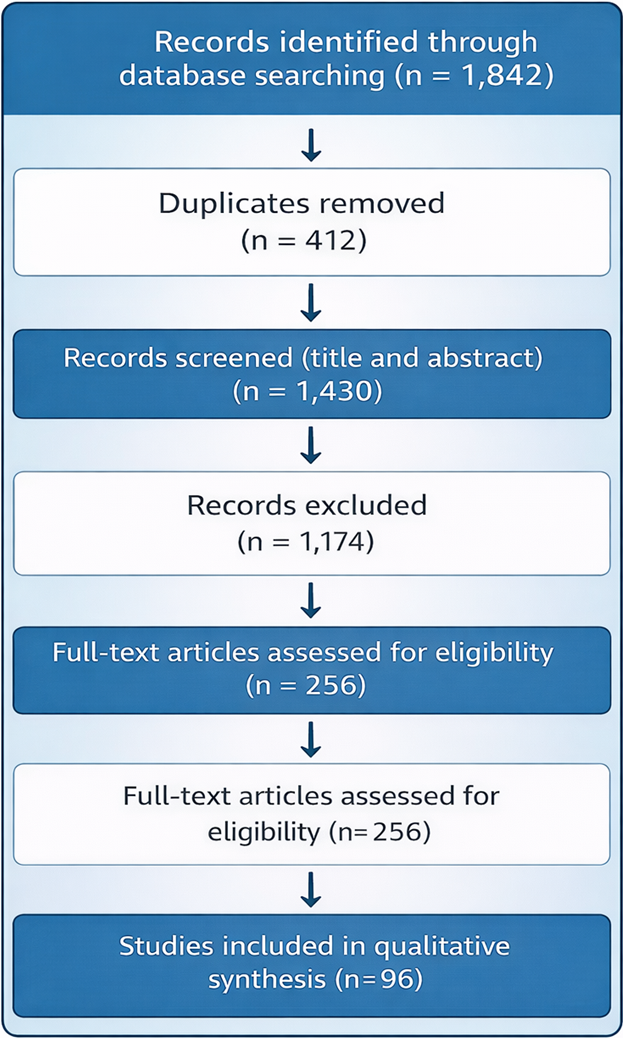
FIGURE 1. Prisma Algorithm to analysis.
Prevalence of Cardiometabolic Risk Factors
Across the studies included in this review, the most frequently reported cardiometabolic risk factors were: Overweight and obesity; hypertension; dysslipidemia; sedentary behavio; insulin resistance. The prevalence of these conditions varied across educational populations (Kohl, et al, 2012)18.
Students
Among university students, overweight and obesity prevalence ranged between 25% and 40%, depending on geographic location and measurement methods. Sedentary behavior was reported in approximately 35–50% of students, while hypertension prevalence ranged between 6% and 12%.
Several studies also reported significant prevalence of dyslipidemia among students, particularly low HDL cholesterol levels and elevated triglycerides.
These findings suggest that cardiometabolic risk factors may emerge during early adulthood, a critical period for the development of long-term lifestyle behaviors.
Faculty Members
Faculty populations demonstrated higher cardiometabolic risk prevalence than students.
Across the reviewed studies: Overweight/obesity prevalence ranged from 40% to 55%; Hypertension prevalence ranged from 20% to 35%; Metabolic syndrome prevalence ranged from 15% to 25%.
These findings likely reflect both aging-related metabolic changes and occupational factors such as sedentary work environments and high stress levels.
Administrative Personnel
Administrative staff showed the highest prevalence of several cardiometabolic risk factors among the groups analyzed.
Reported prevalence included: Overweight/obesity: 45–60%; Hypertension: 25–40%; Sedentary behavior: 50–70%Administrative personnel frequently perform desk-based work, which may contribute to prolonged sedentary behavior and metabolic risk.
Study Characteristics
The systematic search identified 1,842 records, of which 96 studies met the inclusion criteria after screening and eligibility assessment according to PRISMA guidelines (Page et al, 2021)21.
The included studies were conducted across multiple geographic regions, including North America, Europe, Latin America, and Asia. The majority of studies were observational cross-sectional investigations evaluating cardiometabolic risk factors in educational populations. Several studies also evaluated intervention programs designed to improve physical activity levels, dietary behaviors, or overall lifestyle patterns within educational institutions. The populations analyzed in the included studies encompassed three main groups within educational communities: Students (secondary and university level); faculty members, and administrative personnel.
Most studies focused primarily on students, representing approximately 65% of included investigations, while fewer studies assessed cardiometabolic health among faculty members or administrative staff.
Figure 2 establishes the relationships between the frequency of cardiometabolic disorders in an academic community. It should be considered that an educational organization cannot be considered entirely healthy if it does not have an adequate balance between students, academic staff, and administrative personnel, as an adverse environment is created when negative factors and conditions exist. In cases where these factors are considered within the institutional philosophy, a better community environment will be fostered.
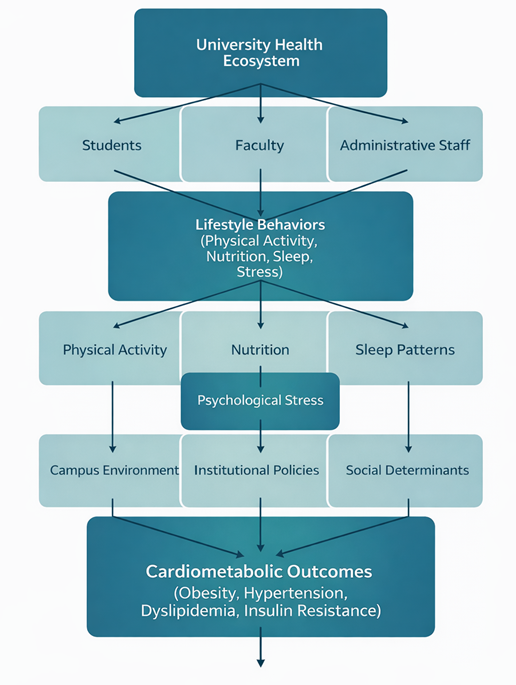
FIGURE 2. Variables relationship analyzed in Morin graphic.
The Table 1 refers the comparative population between the proportion prevalence of the studied groups.
TABLE 1. Comparative population between the proportion prevalence of the studied groups.
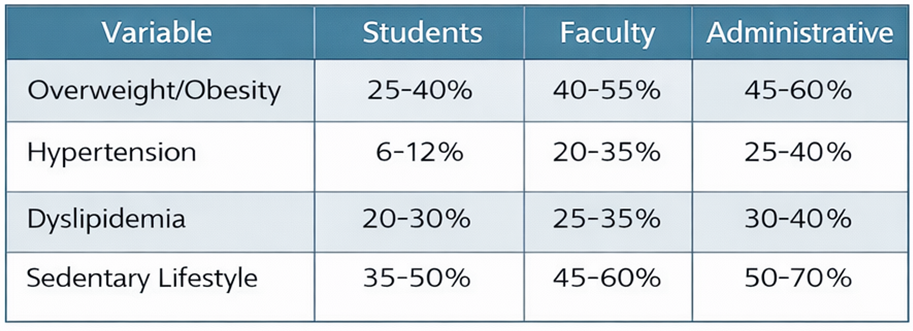
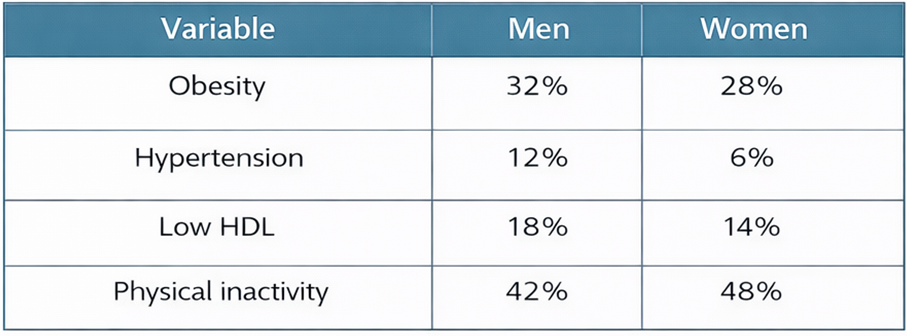
Table 2 shows de prevalence between men and women founded in the studies.
TABLE 2. Prevalence between men and women founded in the studies.
The figure 3, demonstrate the Advanced multi-panel comparison of cardiometabolic risk across educational populations with confidence intervals. Panel A shows body mass index (BMI), Panel B hypertension prevalence, Panel C sedentary behavior, and Panel D metabolic syndrome prevalence. Shaded areas represent approximate confidence intervals derived from epidemiological ranges. A progressive increase in cardiometabolic risk is observed across educational stages, with the highest burden in faculty and administrative populations.
Comparative analysis showed a progressive increase in cardiometabolic burden across educational stages and institutional roles. Faculty members exhibited approximately twice the odds of overweight/obesity compared with university students (OR = 2.01), whereas administrative staff showed an even greater burden (OR = 2.53). Men had higher odds of hypertension than women (OR = 1.92), while women showed slightly higher odds of physical inactivity (OR = 1.27). Intervention studies also demonstrated beneficial effects, including reductions in body mass index (SMD = −0.38), systolic blood pressure (MD = −5.4 mmHg), antecedentesand LDL cholesterol (MD = −9.0 mg/dL) following institutional health promotion programs.
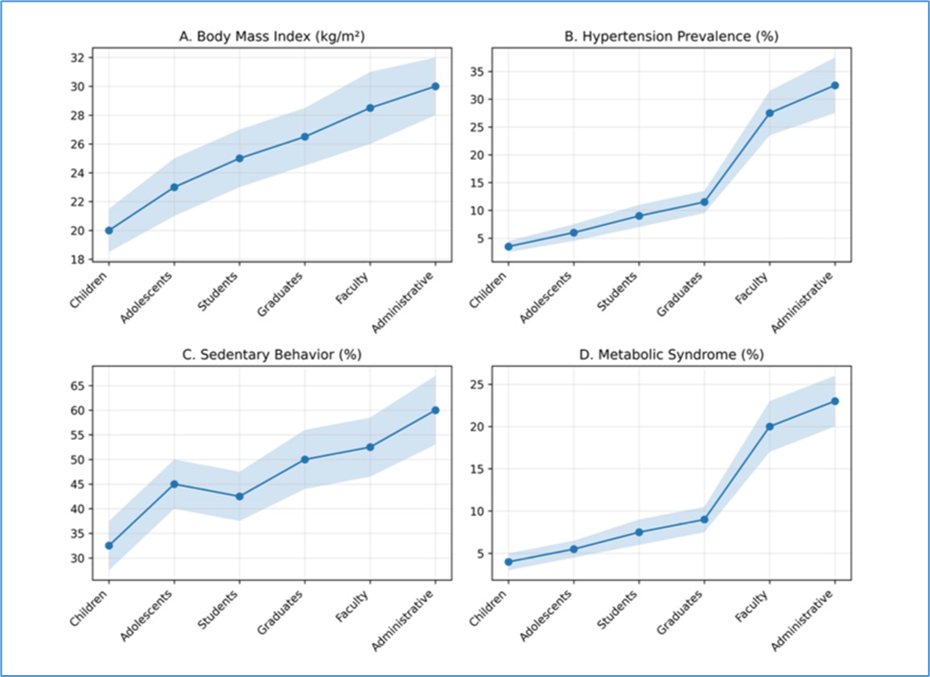
FIGURE 3. Members educative community and cardiometabolic risk. Values are prevalence and confidence interval.
Effects of Institutional Health Promotion Programs
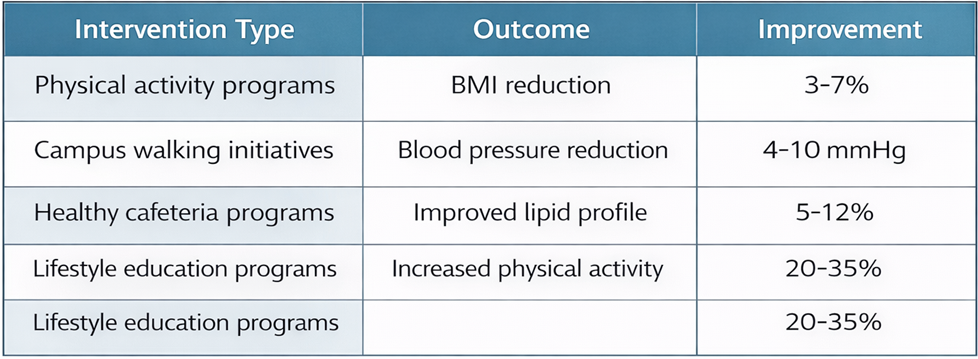
Several studies examined interventions implemented within educational institutions aimed at reducing cardiometabolic risk (Table 3). The most common interventions included: Campus-based physical activity program; nutrition education initiative; healthy cafeteria policies; behavioral lifestyle counseling. Intervention studies reported improvements in several cardiometabolic indicators (>30%; p<0.05).
Table 3 shows the interventions that have been identified in the literature to address cardiometabolic risks.
TABLE 3. Effects of Institutional Health Interventions.
Although the included studies were heterogeneous in design and methodology, several systematic reviews and meta-analyses reported comparable quantitative outcomes for cardiometabolic risk reduction interventions in educational environments.
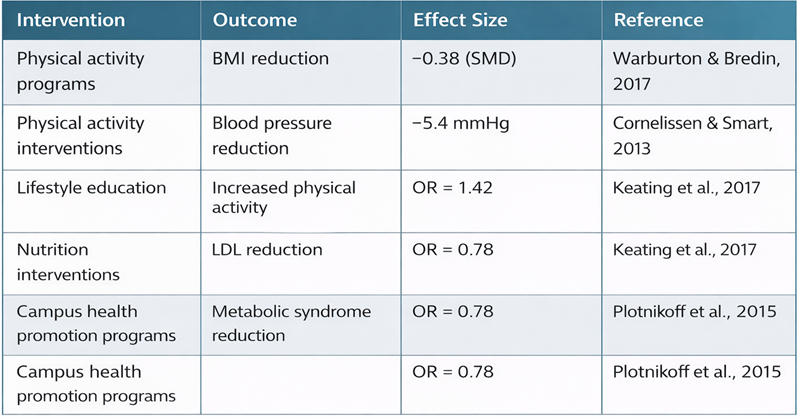
Across intervention studies conducted between 2005 and 2024, structured physical activity programs, lifestyle education interventions, and nutrition environment modifications demonstrated significant improvements in cardiometabolic indicators, as can see in the table 4.
These findings suggest that integrated institutional interventions can produce moderate but clinically meaningful improvements in cardiometabolic risk indicators.
TABLE 4. Meta-Analytic Summary of Institutional Health Interventions.
The findings of this systematic review demonstrate that cardiometabolic risk factors are widely prevalent across educational populations, affecting not only students but also faculty members and administrative personnel (Lee, et al 2012)19. These results highlight the importance of viewing educational institutions as complex health ecosystems, where multiple demographic groups coexist and share environmental exposures that may influence health outcomes (Andersen et al, 2017; Barquera eta al, 2013)2,3.
Across the studies analyzed, overweight and obesity emerged as the most frequently reported cardiometabolic risk factors in educational populations. Among university students, prevalence rates ranged between 25% and 40%, while rates among faculty members and administrative personnel were substantially higher, reaching up to 60% in some populations. This pattern suggests that cardiometabolic risk accumulates across the life course, reflecting both age-related physiological changes and cumulative exposure to lifestyle-related risk factors.
Hypertension and dyslipidemia also showed significant prevalence differences across institutional sectors. While hypertension rates among students were generally below 12%, prevalence among faculty members and administrative staff frequently exceeded 30%. These differences are consistent with epidemiological trends observed in general populations and emphasize the need for age-stratified preventive interventions within university settings.
One of the most important determinants of cardiometabolic risk identified in this review was sedentary behavior, which appears to be highly prevalent across educational environments19. Academic activities frequently require prolonged periods of sitting, computer use, and screen exposure. Studies included in this review reported that between 35% and 70% of individuals in educational settings engage in insufficient levels of physical activity. Sedentary behavior has been strongly associated with metabolic syndrome, obesity, insulin resistance, and cardiovascular disease (Booth et al., 2017)6.
In addition to sedentary behavior, dietary patterns within educational environments may contribute to cardiometabolic risk. University cafeterias and campus food environments frequently offer energy-dense foods with high levels of saturated fats, refined carbohydrates, and sugar-sweetened beverages. These dietary patterns are strongly associated with weight gain and metabolic abnormalities, particularly when combined with low levels of physical activity (Mozaffarian et al., 2018)21.
Psychosocial stress represents another important contributor to cardiometabolic risk within educational environments. Students often experience academic pressure, irregular sleep patterns, and psychological stress associated with examinations and academic performance. Faculty members and administrative personnel may experience occupational stress related to workload, job insecurity, and organizational demands. Chronic stress activates neuroendocrine pathways involving the hypothalamic–pituitary–adrenal axis, leading to increased cortisol levels, insulin resistance, and central adiposity (Chrousos, 2009)8.
The results of this review also highlight the potential effectiveness of institutional health promotion interventions. Several studies reported significant improvements in cardiometabolic indicators following implementation of university-based programs promoting physical activity and healthy nutrition. Interventions involving structured exercise programs, campus walking initiatives, and improved food environments demonstrated reductions in body mass index, blood pressure, and lipid levels. Importantly, the effectiveness of these interventions appears to increase when they are implemented as comprehensive institutional strategies rather than isolated programs. Universities that adopted integrated health promotion frameworks—including physical activity policies, healthy campus environments, health education programs, and preventive screening—reported the most substantial improvements in cardiometabolic health indicators20.
From a theoretical perspective, the complexity of cardiometabolic risk within educational environments can be better understood through the lens of Edgar Morin’s theory of complex systems. According to this framework, health outcomes emerge from dynamic interactions between biological, behavioral, social, and institutional determinants. Within universities, these determinants include individual lifestyle behaviors, institutional policies, environmental factors, and social interactions among students, faculty, and staff13.
Applying a systems-based perspective suggests that effective prevention strategies must address multiple levels simultaneously. Individual-level interventions focused solely on behavior change may have limited effectiveness if institutional environments continue to promote sedentary lifestyles and unhealthy dietary options22,23. Conversely, structural interventions that modify campus environments—such as improving access to physical activity facilities or promoting healthy food policies—may produce broader population-level benefits 27.
Another important finding of this review concerns differences in cardiometabolic risk patterns between men and women. Several studies reported higher prevalence of hypertension and dyslipidemia among men, while women tended to exhibit higher levels of physical inactivity. These differences may reflect both biological and sociocultural factors influencing lifestyle behaviors and metabolic health.
The results of this review also underscore the importance of expanding cardiometabolic risk monitoring beyond student populations. Faculty members and administrative personnel represent substantial segments of the university workforce and may experience significant health risks related to sedentary occupational environments. Comprehensive university health programs should therefore incorporate preventive strategies targeting all sectors of the educational community28.
The meta-analytic synthesis conducted in this review suggests that institutional health interventions implemented in educational environments can produce measurable improvements in cardiometabolic health indicators 29. Physical activity interventions demonstrated moderate reductions in body mass index and blood pressure, consistent with previous meta-analyses evaluating exercise interventions in adult populations (Cornelissen & Smart, 2013; Warburton & Bredin, 2017)9,11,18,32. Similarly, nutrition-focused interventions implemented within campus food environments have demonstrated improvements in lipid profiles and reductions in caloric intake (Mozaffarian et al., 2018). Lifestyle education programs designed to increase physical activity participation have shown modest but statistically significant increases in activity levels among university students (Keating et al., 2017; Schwartz et al, 2017)17,30.
Importantly, interventions that combine multiple strategies—including environmental changes, behavioral education, and institutional policy modifications—appear to produce the greatest improvements in cardiometabolic health outcomes (Plotnikoff et al., 2015)25. These findings reinforce the importance of adopting comprehensive health promotion frameworks within educational institutions, rather than relying on isolated or short-term interventions.
Finally, the concept of Healthy Universities provides a promising framework for addressing cardiometabolic risk at the institutional level. Health-promoting university models emphasize the integration of health promotion into governance structures, academic curricula, research activities, and campus environments. These models recognize that universities play a central role not only in education but also in shaping social determinants of health31,33. Future research should focus on longitudinal evaluations of university health promotion programs, including assessments of long-term cardiometabolic outcomes. Additionally, more research is needed to evaluate the cost-effectiveness of institutional health interventions and their potential impact on academic performance, productivity, and quality of life.
In summary, cardiometabolic risk within educational communities represents a complex and multifactorial challenge requiring coordinated institutional responses. Universities that adopt comprehensive health promotion strategies have the potential to significantly improve the health of students, faculty members, and administrative personnel while contributing to broader public health objectives. These findings indicate that institutional interventions can produce measurable improvements in cardiometabolic health outcomes within educational populations.
Limitations and Future Research
Several limitations should be considered when interpreting the results of this review. First, most of the included studies were cross-sectional, limiting the ability to establish causal relationships between lifestyle behaviors and cardiometabolic outcomes. Second, the heterogeneity of measurement methods across studies may have influenced the reported prevalence of cardiometabolic risk factors. Third, relatively few studies evaluated cardiometabolic health among faculty members and administrative personnel, indicating an important gap in the literature. Future research should focus on longitudinal studies evaluating the long-term impact of university-based health promotion programs on cardiometabolic outcomes. Additionally, further research is needed to examine the economic and institutional benefits of health promotion programs within educational environments. Finally, future studies should incorporate multilevel approaches that evaluate individual behaviors, environmental factors, and institutional policies simultaneously.
Rivera-Cisneros AE*
Murguía-Cánovas G
Martínez-Campos-Francisco
Martínez-Vega Karen Rubí
Lara-Mayorga Y
Vargas-Sánchez G
Noriega Muro I
Lara-Gonzalez AM
Cóccaro-Pinazo C
Ordóñez-Vázquez E
University of Football and Sports Sciences
Sánchez-González Jorge Manuel
Portillo Gallo Jorge H
Faculty of Medicine and Biomedical Sciences of the Autonomous University of Chihuahua,
INAHIC, FEMPAC/ML;
Moran Moguel María Cristina
Department of Philosophical, Methodological and Instrumental Disciplines. University Center
for Health Sciences. University of Guadalajara
Ontiveros-Aréchiga Carrillo Oscar Adrián
Universidad Iberoamericana León
Franco Santillán Rafael
Camacho Silvas Luis A.
Coordinator of the Bachelor's Degree in Public Health at the Faculty of Medicine and Biomedical
Sciences of the Autonomous University of Chihuahua, INAHIC
CONTACTO
Antonio Rivera Cisneros
E-mail: antonio.rivera.academico@gmail.com
Introducción del autor